Contents of Article
- Summary
- What is growth?
- Why is monitoring growth important?
- How do you monitor growth?
- Are there any issues with monitoring growth?
- Considerations for monitoring growth
- Conclusion
- About the Author
- References
Summary
All humans experience growth during the early stages of life. For youth athletes, body composition and size are often a predictor of strength and power when relative to chronological age. Sports performance professionals may find it useful to monitor anthropometrics, such as height and weight, in order to determine periods of peak growth within a child’s development.
Alternatively, it is just as critical to determine periods of stunted growth. A child experiencing normal growth relative to their age group is likely to be in good health, meanwhile, a child experiencing abnormal growth may have an underlying disease or hormonal problem, for example. Early identification of a growth problem should be made known to a medical professional. The earlier the detection, the more effective treatment can be for a child to assist with healthy development.

What is growth?
Growth is a natural and individual biological activity all humans go through, starting from conception up until adulthood. Noticeable changes can be seen in the body during the first 20 years or so of life. Bones and muscle tissue grow within our body parts which results in an increase in height and weight.
Physiologically speaking, growth is a multi-factorial process but happens due to a combination of hyperplasia, hypertrophy, and accretion [1]. These cellular processes drive growth in a non-linear path from childhood until adulthood [1]. We not only see growth in tissue, but also in behavioural, cognitive, and social characteristics.
Why is monitoring growth important?
Assessing a child’s height is a great indicator of their general health [2]. When a child experiences abnormal growth, this may indicate the child has a disease or health condition that can affect their final adult stature or wellbeing [2]. Early detection of abnormal growth allows for an appropriate medical diagnosis, and in some cases, may even be treatable [2]. The later a growth problem goes unrecognised/unreported, the opportunities for medical assistance for that child decreases.
Most countries have different standards for assessing short stature and abnormal growth which is relevant to their population. For example, in the UK, a child’s height below the 0.4th percentile is assigned as severe short stature [3]. While in the Netherlands, severe short stature is anything greater than -2.5 standard deviations from the norm [4]. Although this accounts for a small portion of each country’s population, the fact remains that assessment of children’s height should be assessed against normative growth reference charts for identification.
In 2004, The World Health Organization (WHO) assessed the growth and development of young children all over the world [5]. Specifically, they studied 8,440 children from six countries of diverse cultural and ethnic backgrounds (Brazil, Ghana, India, Norway, Oman, and the USA) to more comprehensively understand growth. Their findings report that healthy children are more likely to reach their full genetic potential when living under healthy conditions which include: nutrition, BMI, breastfeeding, and parents refraining from smoking. While broad, this indicates that regardless of ethnicity, socioeconomic status, or type of breastfeeding, children can grow normally when living in optimal healthy conditions.
As alluded to previously, all children do not grow at the same rate, nor in a linear fashion. As a result, it is crucial that all sports performance professionals, understand if an athlete is growing at a “normal” rate, or if, for some reason, their growth appears to be “abnormal” (e.g. stunted). By measuring growth rates on an ongoing basis, the coach/practitioner will be able to identify if an athlete is experiencing a period of “abnormal” growth, and being able to do so could be vital for that child’s health and performance.
Though the coach/practitioner may be capable of identifying whether or not an athlete might be experiencing a period of abnormal (e.g. stunted) growth, they cannot, and should not, attempt to diagnose the issue themselves. Instead, the coach/practitioner needs to make an educated and strategic decision regarding the proceeding course of action; for example, notifying the parent(s) and/or a qualified medical practitioner.
The reason for this is simply because a child’s growth may be abnormal (e.g. stunted) for myriad complex reasons. Some of these may include:
- Genetic predisposition (e.g. Achondroplasia)
- Malnutrition
- Illness (e.g. thyroid disease)
- Endocrine disorders
- Injury (e.g. damage to the epiphyseal plates in bones)
In some cases, for example, the coach/practitioner may not want to inform the parent(s) directly as the issue could be the result of malnutrition which may have arisen from issues at the child’s home (e.g. domestic abuse). Collectively, all of this information highlights the severity and complexity of potential problems surrounding a child’s growth.
How do you monitor growth?
Monitoring growth is a simple and practical task that coaches can implement into training times. However, it may be unnecessary to do so every session. Collecting height and weight data every three months can provide a sufficient picture of the development of an adolescent athlete.
For validity and reliability purposes, the procedures for collecting the data should be similar every time it is performed and with the same equipment. For example, using the same weight scale and stadiometer each time can limit the variance of data. Also, wearing minimal clothing and removing shoes can provide a more accurate estimation of height and weight.
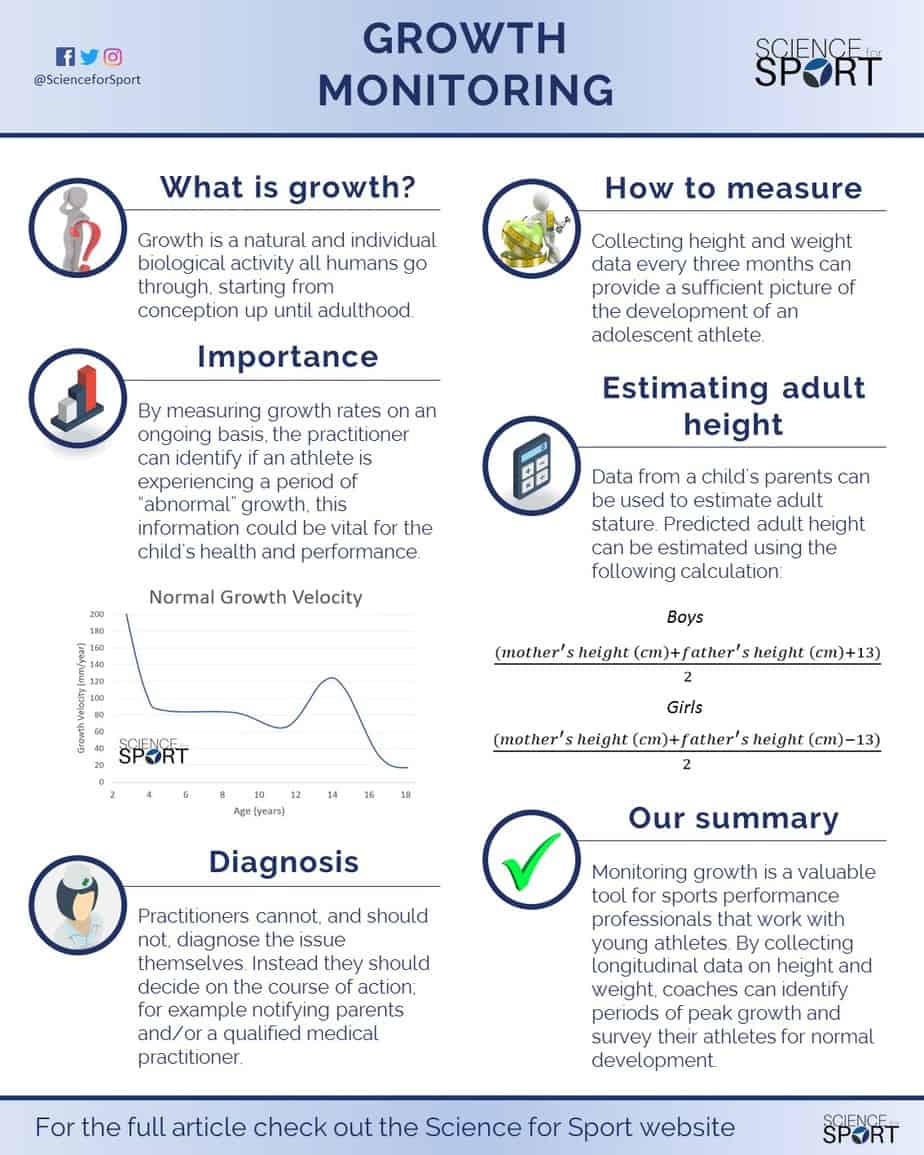
Anthropometric data from a child can be used to estimate adult stature. Predicted adult height can be estimated for individuals if information about the biological parents’ height is obtainable [6]. The equations for both genders can be seen below (Figure 1). Further work by Sherar et al. (2005) [7] concluded that using other anthropometric data such as weight, height, and sitting height to predict adult stature is accurate within 5-8 cm in boys and 3-8 cm in girls for 95 % of cases. The importance of this is that it can be combined with longitudinal growth and determine the percentage of predicted adult stature.

If you’d like to know more about predicting an athlete’s adult stature, then you can read our article on bio-banding and download your FREE adult stature prediction spreadsheet (named: Bio-Banding Calculator) which you can use right away with your athletes.
Click HERE to read the article and get your FREE Bio-Banding Calculator.

Are there any issues with monitoring growth?
Keeping longitudinal data on height and weight allows coaches to identify peak growth rates, only after they have already occurred. For this reason, monitoring growth on its own may not provide enough information for coaches, therefore, it is recommended that this is combined with other data to determine maturity offset (e.g. peak-height velocity (PHV)) or growth velocity.
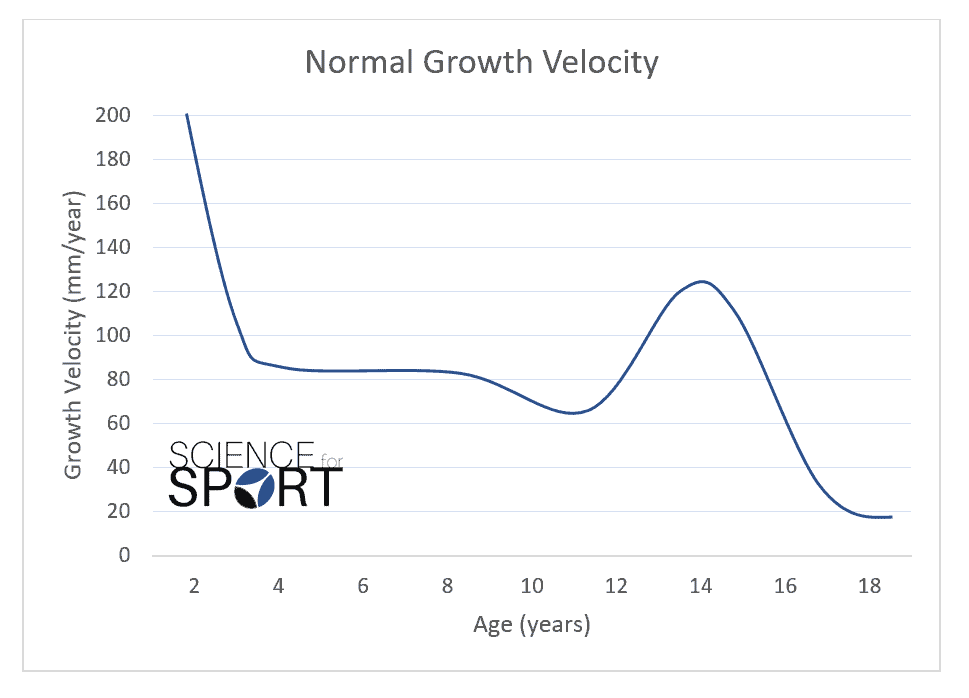
Growth velocity is the rate of growth over time (millimetres per year (mm/year)) that young humans experience. A typical growth velocity curve shows fast growth in early childhood, then gradually slowing down until the start of the pubertal growth spurt (Figure 2). During the decline from infancy to late adolescence, it is not unusual for a young child’s height to be in the 95th percentile one month and be in the 20th percentile the next [2]. Human growth can be highly complex, which can make interpretation difficult.
This huge variation in growth should not be of concern unless an infant is assessed below the 5th percentile in consecutive measurements over a period of 3-6 months [2]. If an athlete is referred to a medical practitioner for short stature, the physician will generally adopt a “wait and see” policy over a short period of time before recommending specialist advice or treatment [8].
Misdiagnosis of growth disorders and unnecessary referrals can arise from errors in height measurement or inaccurate plotting of values in a growth chart [2]. For this reason, it is critical to assess a child’s height consistently with the same reliable tools and methods. Also, having an appropriate growth chart can be an essential tool for surveillance of a child’s height.
Patterns of growth are different between genders after puberty [9]. Pre-puberty, body composition is similar between genders but changes at the onset of puberty due to more circulating androgens in boys compared to girls [1]. During the adolescent growth spurt, boys tend to experience greater increases in arm girth and shoulder width compared to girls [10]. Also, boys tend to have greater fat-free mass and about half the body fat percentage to that of girls at the end of the adolescent growth spurt. Meanwhile, girls tend to experience greater increases in hip width and fat mass compared to boys [1].
Considerations for monitoring growth
Monitoring growth is simply that – do not diagnose. If a child appears to fall out of the 5th or 95th percentile for growth at their age, the best thing to do may be to refer out to qualified medical practitioners (e.g. physician). Growth is multi-factorial and can be influenced by many factors such as genetics, malnutrition, or damage to the epiphyseal plates in bones.
As coaches, we should not overstep our boundaries and improperly diagnose athletes. Monitoring growth gives us critical information about the development of an athlete but does not reveal the underpinning factors that may cause it.
Conclusion
Monitoring growth is a valuable tool for sport performance professionals who work with young athletes. By collecting longitudinal data on height and weight, coaches can identify periods of peak growth and survey their athletes for normal development.
Coaches who identify children who fall outside of the normative height or weight values for their chronological age group should refer to qualified medical practitioners (e.g. physicians). From there, medical professionals can supply children with appropriate treatments which can optimise the possibility for good health, and development, and therefore towards reaching their optimal adult height.
- Lloyd, RS and Oliver JL. Strength and Conditioning for Young Athletes: Science and Application. Routledge, 2014. https://www.amazon.co.uk/Strength-Conditioning-Young-Athletes-Rhodri/dp/0415694892
- Haymond, M., Kappelgaard, AM., Czernichow, P., Biller, BM., Takano, K., Kiess, W. (2013). Early Recognition of Growth Abnormalities Permitting Early Intervention. Acta Paediatr 102(8): 787-796. https://www.ncbi.nlm.nih.gov/pubmed/23586744
- National Screening Committee. National Screening Committee policy- growth screening. Avaliable at: http://www.screening.nhs.uk/growth (accessed on March 25, 2017).
- Grote, F., Oostdijk, W., De Muinch Keizer-Schrama, S., van Dommelen, P., van Buuren, S., Dekker, F. (2008). The Diagnostic Work Up of Growth Failer in Secondary Health Care; An Evaluation of Consensus Guidelines. BMC Pediatr 8-21. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2422838/
- de Onis, M., Garza, C., Victora, C., Onyango, A., Frongillo, E., Martines, J. (2004). The WHO Multicentre Growth Reference Study: planning, study design, and methodology. Food Nutr Bull 25(1) 15-26. https://www.ncbi.nlm.nih.gov/pubmed/15069916
- Tanner, J., Goldstein, H., Whitehouse, R. (1970). Standards for children’s height at ages 2-9 years allowing for heights of parents. Archives of Disease in Childhood. 45: 755-762. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1647404/
- Sherar, L., Mirwald, R., Baxter-Jones, A., Thomis, M. (2005). Prediction of adult height using maturity-based cumulative height velocity curves. Journal of Pediatrics. 147: 508-514. https://www.ncbi.nlm.nih.gov/pubmed/16227038
- Ahmed, ML., Allen, AD., Sharma, A., Macfarlane, JA., Dunger, DB. (1993). Evaluation of a district growth screening programme: The Oxford Growth Study. Arch Dis Child 69(3) 361-365. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1029521/
- de Onis, M., Onyango, A., Borghi, E., Siyam, A., Blossner, M., Lutter, C. (2012). Worldwide implementation of the WHO Child Growth Standards. Public Health Nutr 12: 1-8. https://www.ncbi.nlm.nih.gov/pubmed/22717390
- Malina R.M. et al., (2004) Maturity-associated variation in the growth and functional capacities of youth football (soccer) players 13–15 years. European Journal of Applied Physiology, Volume 91, Issue 5–6, pp 555–562. https://link.springer.com/article/10.1007/s00421-003-0995-z

